Шталь про кветиапин, часть 2, сравнение обычной и пролонг версии. Пришлось немного сжать изображение, потому что оно не загружалось. Вложение:
 IMG_4500.jpeg [ 132.63 КБ | Просмотров: 3648 ]
IMG_4500.jpeg [ 132.63 КБ | Просмотров: 3648 ]
Мой пересказ:

нажмите, чтобы увидеть
Кветиапин в "антидепрессивной" дозировке 300мг показывает очень быстрые результаты в борьбе против биполярной депрессии в сравнении с остальными НЛ и НТ. Основной механизм антидепрессивного действия квета - блокада обратного захвата норадреналина и антагонизм к 5-НТ-2С рецептору, что вызывает повышение уровня норадреналина и дофамина в ЦНС. Также помощь в борьбе с биполярной депрессией оказывает частичный агонизм к 5HT1А, антагонизм к 5HT7, α2, 5HT1B/D.
Комбинация кветиапина с СИОЗСН вызовет мощное повышение уровней всех 3 нейромедиаторов, при этом будет решена проблема бессонницы и тревоги за счет антигистаминного механизма.
Дозировка в 300мг оказывает антидепрессивный эффект такой же силы, что и дозировка в 600мг.
В средних и высоких дозах кветиапин провоцирует инсулинорезистентность и повышение уровня триглицеридов в крови.
Оригинальный текст Шталя:
нажмите, чтобы увидеть
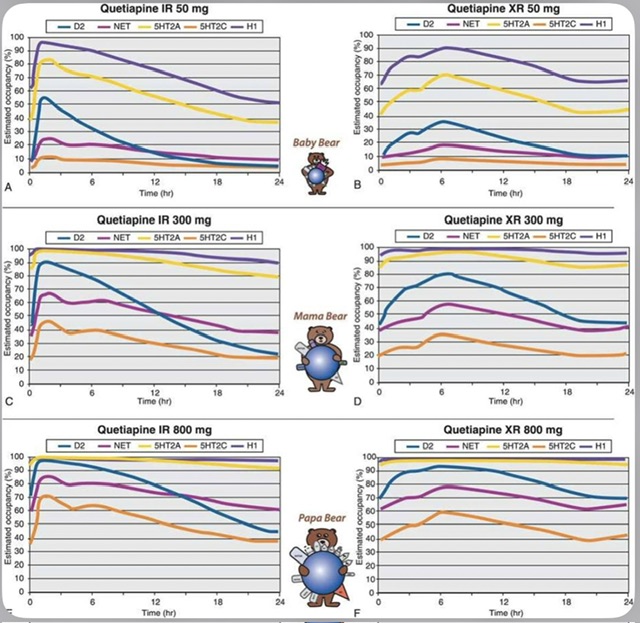
Figure 5-50. Binding profile of quetiapine with different doses and formulations. (A, B) The estimated receptor occupancy for quetiapine IR and XR at 50 mg/day is shown here. Although quetiapine binds to multiple receptors at this dose, its most prominent action is at histamine 1 receptors, thus explaining its use as a sedative-hypnotic at this dose. (C, D) At antidepressant doses, histamine 1 and 5HT2Aantagonism are the most prominent binding properties of both quetiapine IR and XR, with additional binding at D2 receptors, the norepinephrine transporter, and 5HT2C receptors. (E, F) At antipsychotic doses, the strongest binding properties of quetiapine IR and XR are also histamine 1 and 5HT2A antagonism. However, occupancy at the D2 receptor, norepinephrine transporter, and 5HT2C receptor is greater than at lower doses.
Mama Bear is the surprise bear in many ways. Although developed as an antipsychotic, quetiapine was anecdotally observed to have antidepressant effects in bipolar and unipolar depressed patients, beyond helping them sleep, and in the absence of psychotic symptoms. Over time, clinical trials have repeatedly demonstrated that in the 300 mg range, quetiapine has some of the most robust antidepressant effects of any agent in bipolar depression. At first, this did not make any sense pharmacologically for a 5HT2A–D2 antagonist with antihistaminic properties, but then the active metabolite norquetiapine was discovered with its norepinephrine reuptake blocking and 5HT2Cantagonist properties, much greater than for the parent quetiapine itself. These two mechanisms can individually increase the release of both dopamine and norepinephrine, and together appear to have synergistic actions at doses below those that cause 60% D2 occupancy (Figure 5-50C and D). In addition, quetiapine has 5HT1A partial agonist, 5HT7, α2, and 5HT1B/D antagonist properties, also theoretically linked to antidepressant actions. These multiple concomitant pharmacological actions theoretically have accounted for ushering in the arrival of antidepressant quetiapine, a 300 mg Mama Bear. This constitutes a big paradigm shift for a drug originally developed as an antipsychotic for schizophrenia. Although both the IR (Figure 5-50C) and XR (Figure 5-50D) formulations appear to have antidepressant efficacy, the XR formulation has more consistent day-long receptor occupancy of both 5HT2Creceptors and norepinephrine transporters as well as other key receptors, and may thus be theoretically the preferred formulation for the treatment of depression. Quetiapine is approved both for bipolar depression and as an augmenting agent to SSRIs/SNRIs in unipolar depression that fails to respond sufficiently to SSRI/SNRI monotherapy. Thus, the combination of quetiapine with these other antidepressants in unipolar treatment-resistant depression would have the triple monoamine actions of increasing serotonin (via SSRI/SNRI actions), dopamine, and norepinephrine (the latter two neurotransmitters theoretically via quetiapine/norquetiapine 5HT2C antagonist actions plus both quetiapine and SNRI prefrontal cortex NET blockade), while simultaneously treating symptoms of insomnia and anxiety by antihistaminic action (Figure 5-50C and D).
Finally, Papa Bear is 800 mg quetiapine, which completely saturates both H1-histamine and 5HT2A receptors continuously in both cases, but has more consistent occupancy above 60% for D2 receptors with the XR formulation (compare Figure 5-50E and F). Substantial occupancy of the antidepressant-related receptors also occurs with either formulation, but this amount of 5HT2C and norepinephrine transporter blockade is not necessary for antidepressant actions, since most studies show that even 300 mg once a day has the same antidepressant efficacy as 600 mg. The 800 mg dose (Figure 5-50E and F) is really an antipsychotic dose, and potentially excessive and less well tolerated for the treatment of depression.
No matter what the dose or the formulation, quetiapine is “very atypical” in that it causes virtually no EPS at any dose, nor prolactin elevations. Thus, quetiapine tends to be a preferred atypical antipsychotic for patients with Parkinson's disease who require treatment for psychosis (as is clozapine). Quetiapine can cause weight gain, particularly when given in moderate to high doses, as it blocks histamine 1 receptors (Figure 5-47); the 5HT2C antagonist actions of its active metabolite norquetiapine may contribute to weight gain at moderate to high doses of quetiapine (Figure 5-47). Quetiapine can increase fasting triglyceride levels and insulin resistance, particularly at moderate to high doses, and with intermediate to high risk compared to other atypical antipsychotics, possibly via the same unknown pharmacologic mechanism postulated to be active for some other atypical antipsychotics (receptor X in Figures 5-42 and 5-47).
__________________________________
Вакцина уносила от Кунцево до Кузьминок, от Люберец до Химок, на Кузне и между двух Ордынок,
Медицина проносилась мимо... Rest In Peace, покойся с миром.
|











 Инструкции к лекарствам всерьез лучше не воспринимать.
Инструкции к лекарствам всерьез лучше не воспринимать.

 Я просто КПТСР только вот в этом году решила трогать, книжки, вон, купила (
Я просто КПТСР только вот в этом году решила трогать, книжки, вон, купила (  Но он точно работает аналогично, уверен если исследования копнуть, их есть там.
Но он точно работает аналогично, уверен если исследования копнуть, их есть там.


 Падение с высоты для меня были самыми страшными страхами. Надеюсь ты понимаешь, что обсессии как бы специально "выдают" тебе такое, они не имеют ничего общего с твоей личностью, ни откуда ты не спрыгнешь и не суициднешься.
Падение с высоты для меня были самыми страшными страхами. Надеюсь ты понимаешь, что обсессии как бы специально "выдают" тебе такое, они не имеют ничего общего с твоей личностью, ни откуда ты не спрыгнешь и не суициднешься.
 Он стоит дороже всей остальной терапии. Куплю 1 пачку и подожду турецкого. Или всё же Сейзар 200 пить
Он стоит дороже всей остальной терапии. Куплю 1 пачку и подожду турецкого. Или всё же Сейзар 200 пить  но стратегии не особо мое, я книжки по вселенной читала.
но стратегии не особо мое, я книжки по вселенной читала.